
{kind=link}
TLDR: The current advice that LDL is “bad cholesterol”, appears to be outdated, and the actual situation is more complex. In people over 60 high LDL appeared to be protective for mortality.
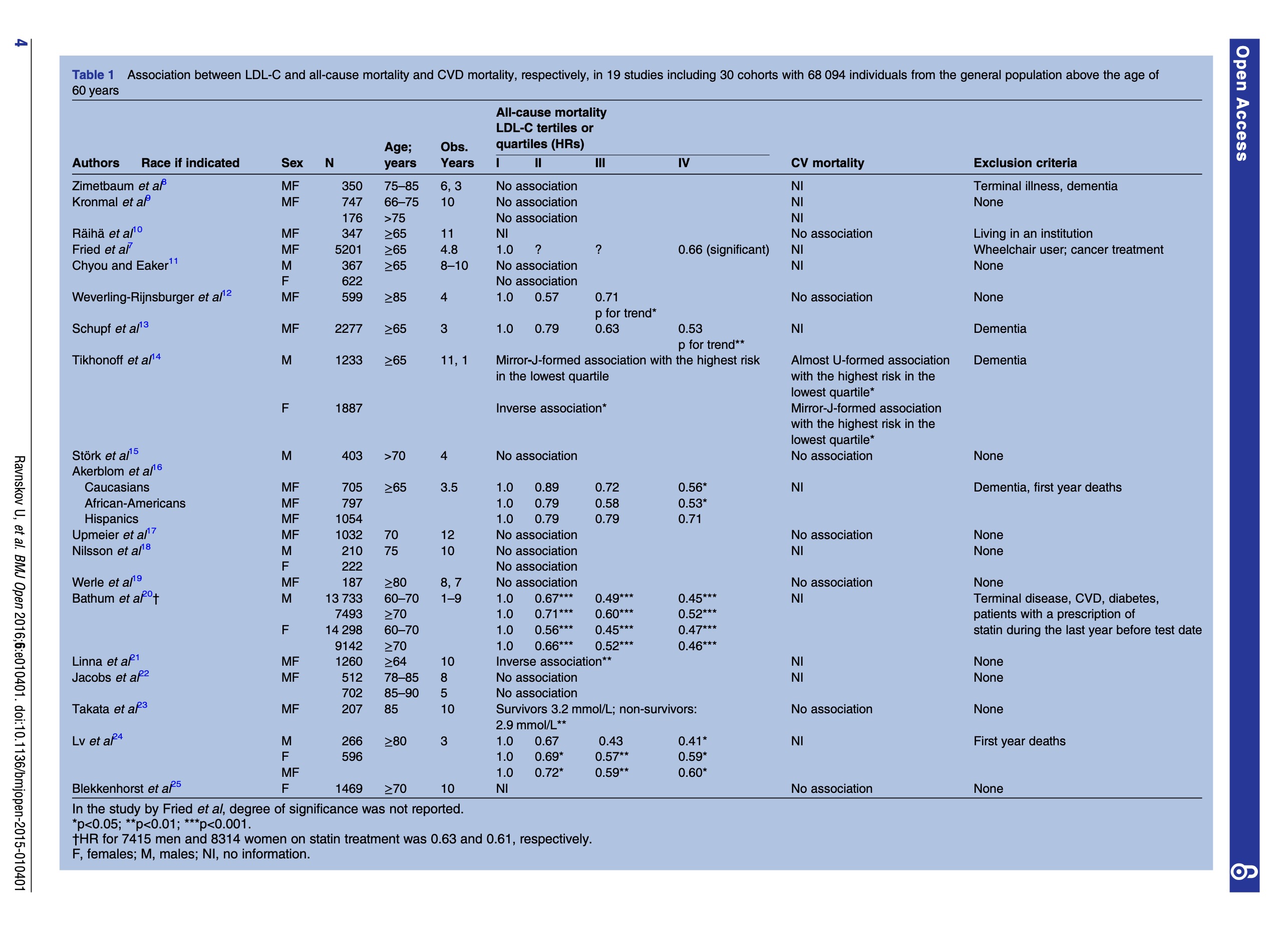
Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies.
Full Paper at https://pubmed.ncbi.nlm.nih.gov/27292972/
Related to, and following up on the LMHR paper from https://hackertalks.com/post/5835924
.
Notes:
The bad cholesterol hypothesis is showing its age, and does not account for mortality data.
The great thing about looking at mortality and LDL measurements is its not a FFQ! So there is less debate about the reality of the study participants.
LDL was seen as PROTECTIVE in 92% of the participants!!! In two studies low LDL was a risk factor for bad endpoints.
ha, thats a academic burn! Side eye on the RR trumpets for small real benefit.
So LDL is protective (1.35 HR which is nothing, but the case against LDL is made with LOWER HRs)
This makes sense, the body makes cholesterol to function, its necessary, a diet that attacks the functioning of cholesterol should have some negative impact on mortality.
I think this is a direct calling out of pharmacological corruption medicine, but said through a academic lens.
LDL are the firemen in our city, and they go where the fire is, you reduce the firemen your going to have a bad time.
The shade in this paper!
Systematic Review of published cohorts, high value science.
evidence pyramid
.