
TLDR: The current advice that LDL is “bad cholesterol”, appears to be outdated, and the actual situation is more complex. In people over 60 high LDL appeared to be protective for mortality.
Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies.
Full Paper at https://pubmed.ncbi.nlm.nih.gov/27292972/
Related to, and following up on the LMHR paper from https://hackertalks.com/post/5835924
.
So this was published almost a decade ago. Has there been any consensus since then? I have not heard about anything other than the standard approach to reducing cholesterol from my doctor.
Consensus? No.
More research, yes: https://www.dietdoctor.com/cholesterol/elevated-ldl-cholesterol
One of the big problems with the lipid hypothesis, is its based on very low relative risk, not absolute risk. And I think the even bigger problem, is pharmacological interests make a lot of money from selling drugs, so they send out the sales reps to tell all the doctors about the research that promotes the use of the drug. There is no nutritional consensus outside of the pharmacy reps, there’s barely any money going into nutrition research outside of industrial investment which is already biased.
Ancel Keys has done a huge disservice to humanity, with his fraudulent research. He threw away data that didn’t fit his theories, he cherry picked data to include to promote his theories. Whatever you want to call what he was doing, it wasn’t science.
https://www.dietdoctor.com/the-hidden-truth-behind-ancel-keys-famous-fat-graph
Well, that’s not comforting for someone with familial hypercholesterolemia. Is LDL > 200 better or worse than taking a statin and ezetimibe in my 30’s? (I don’t expect you to answer that.) Right now I have a doctor who treats high cholesterol by the book without giving it too much thought. I wonder if I should find someone else who is interested in considering these publications.
So, any doctor that just looks at LDL and says “number high, you take statin” needs to be roundly shamed and sent off to the reeducation camps. This has not been the consensus for decades and modern risk stratification tools generally don’t even take into account LDL and instead use a HDL/Total chol ratio.
What is uncontroversial is that statins reduce risk in people who are already at moderate to high risk of cardiovascular events, ideally initially with risk stratification tools like ascvd and followed up with coronary artery calcium scoring or angiography if required.
For FH in particular statins do dramatically reduce risk of CV events.
The cumulative incidence of cardiovascular events and of death from cardiovascular causes at 39 years of age was lower among the patients with familial hypercholesterolemia than among their affected parents (1% vs. 26% and 0% vs. 7%, respectively).
20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia NB. The children took statins, their parents didn’t.
Your doctor may know all this or they may be a quack who is right by accident. I’d guess the former, I’ve been a doctor for a decade and was taught the above in medical school.
Really well said!
HDL/Total chol ratio.
I thought the TG/HDL ratio was the gold standard now. I.e. https://hackertalks.com/post/5922188
Looks like that paper is looking at TG/HDL as a marker for insulin sensitivity and MetSy which is a related but distinct kettle of fish.
20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia
I read the paper, thanks for the link! I found it interesting.
The basis of the available evidence, the LDL hypothesis is no longer a hypothesis and can be considered a fact.16,17 In addition, mendelian randomization studies show that the consequences of LDL cholesterol with respect to the development of atherosclerotic vascular disease are determined not only by the absolute LDL cholesterol level but also by the cumulative exposure of the arterial wall to LDL cholesterol
The paper doesn’t make it clear if this is a statement with respect to FH, or humans in general. One caveat that comes to mind is this statement is lumping in all types of LDL
It is caused by mutations in genes encoding key proteins involved in the low-density lipoprotein (LDL) receptor endocytic and recycling pathways that lead to decreased cellular uptake of LDL cholesterol.
From the introduction of the paper, they define FH as miscoded lipoproteins. I’m not sure the LDL in FH is compatible to non-miscoded LDL (normal people, not glycated, or oxidized), at least in so far as making the first statement a “fact”
From Non-coronary heart disease mortality and risk of fatal cancer in patients with treated heterozygous familial hypercholesterolaemia: a prospective registry study - Full paper is on scihub
Admittedly this study is 10 years older
table 3
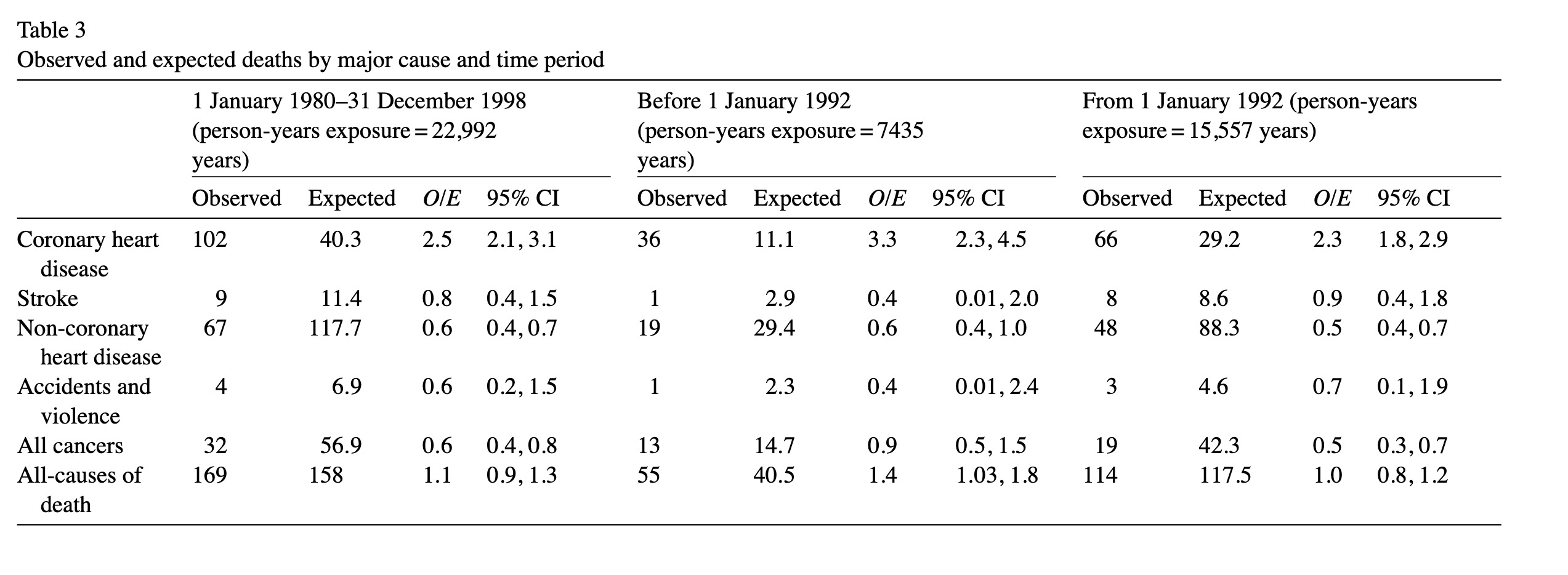
Table 5 is also really interesting.
although coronary mortality remained elevated with statin treatment, all-cause mortality after 1991 did not differ from that of the general population. This was due mainly to an unanticipated 50% decrease in the risk of fatal cancer.
After statin availability subjects with FH appear to have less cancers then the general population. I wonder if this suggests that while very high LDL can be a CVD risk factor, could it also be a cancer risk factor? The authors suggest the cancer reduction is due to lifestyle advice given, but I think it could be suggestive of a impact of LDL. Or was the elevated LDL while being treated with statins protective?
A conversation about cholesterol in another community reminded me I needed to review this paper off my backlog.
https://hackertalks.com/post/6005633/6295546
When we see the flip flopping of advice I think it tells us the science is inconclusive or the relationship noisy.
https://pubmed.ncbi.nlm.nih.gov/27292972/ Here is a systematic review from 2016 saying high LDL is protective vs low LDL, which goes against the current lipid hypothesis - I just point this out because it goes to your point that the advice given flip flops!
This was a good video, but the core question is does LDL CAUSE atherosclerosis or is it associated with atherosclerosis? The video above even says the body will make LDL regardless of diet, so its clearly biologically necessary (that is to say LDL is not a disease). Bad Cholesterol is a poor name for LDL since it is biologically necessary.
There is literature currently saying decreasing LDL has a very small, but real risk reduction across a large population. But since its such a weak signal, I think LDL is a correlated biomarker and not the cause of atherosclerosis. i.e. If every fire you see has firefighters, you might start to think that firefighters start fires.
In the literature there are much stronger hazards to cardiovascular outcomes then LDL, such as metabolic dysfunction, diabetes, hypertension, etc. And very importantly differentiating healthy LDL that gets reused, vs damaged (glycated, oxidized) LDL
LDL is a risk factor, but it should be one datapoint in a panel (obesity, insulin sensitivity, hyper tension, CAC scores!!!, previous CVD events), not just a biomarker people try to treat in isolation.
If this is of interest, I recommend reading this writeup on LDL, its very balanced and cites its sources with confidence scores (the little numbers) https://www.dietdoctor.com/cholesterol/elevated-ldl-cholesterol
.
I do think there is a case for lowering LDL - in patients with advanced atherosclerosis, where the LDL combined with plaque might prevent blood flow. In this limited scenario it is a net positive. Don’t treat the metric (LDL), treat the disease (atherosclerosis). Demand a CAC (Coronary Artery Calcium Scan) before starting on medication that has huge metabolic implications (statins).
firefighter example
https://www.youtube.com/watch?v=2bqkDjVyu80
If your body is already on fire, you don’t want the firemen blocking the roads causing everything to seize up
.
Notes:
The bad cholesterol hypothesis is showing its age, and does not account for mortality data.
The great thing about looking at mortality and LDL measurements is its not a FFQ! So there is less debate about the reality of the study participants.
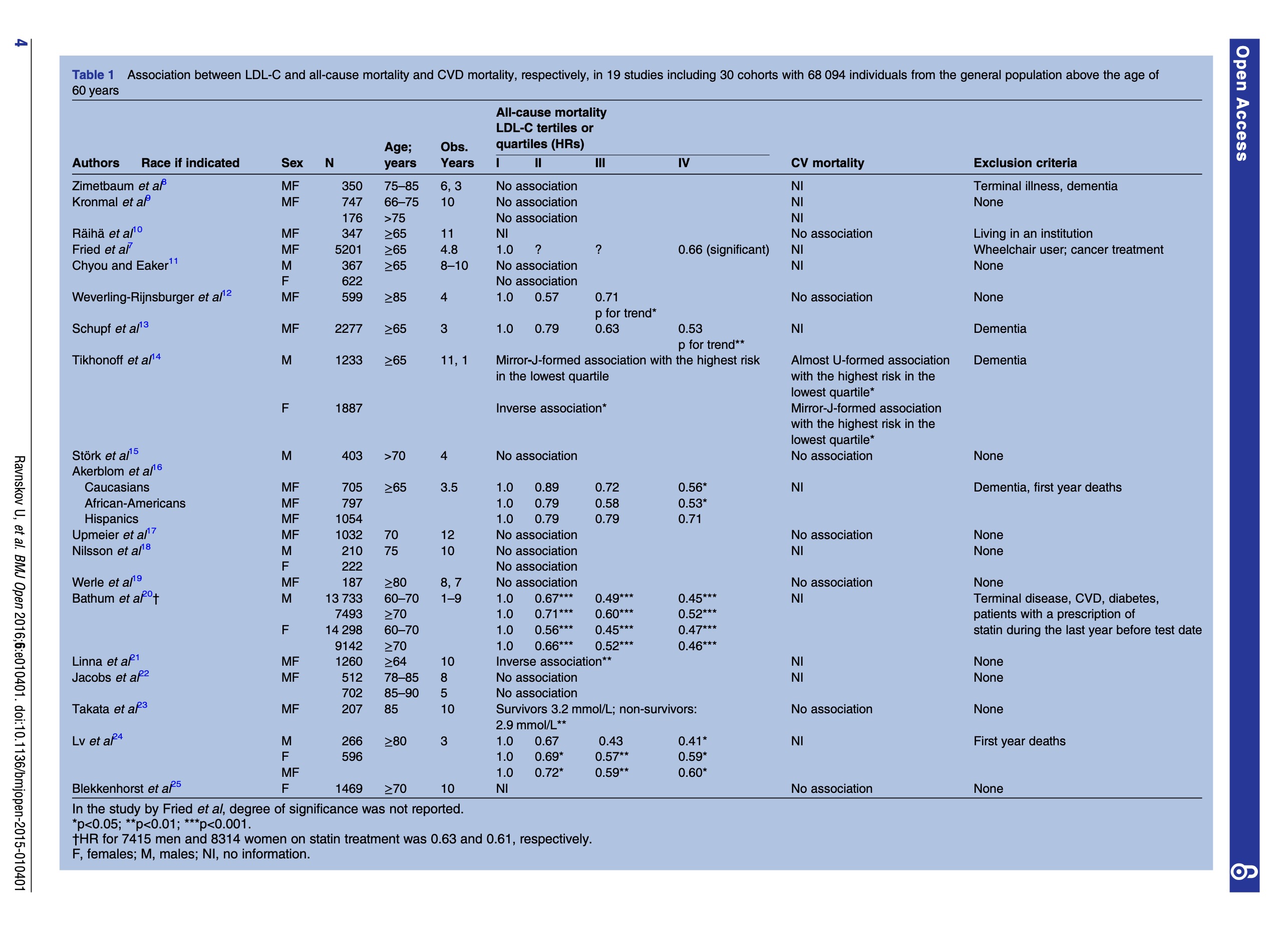
We identified 19 cohort studies including 30 cohorts with a total of 68 094 elderly people, where all-cause mortality was recorded in 28 cohorts and CV mortality in 9 cohorts.
Inverse association between all-cause mortality and LDL-C was seen in 16 cohorts (in 14 with statistical significance) representing 92% of the number of participants, where this association was recorded. In the rest, no association was found. In two cohorts, CV mortality was highest in the lowest LDL-C quartile and with statistical significance; in seven cohorts, no association was found.
LDL was seen as PROTECTIVE in 92% of the participants!!! In two studies low LDL was a risk factor for bad endpoints.
Some of the participants with high LDL-C may have started statin treatment during the observation period and, in this way, may have added a longer life to the group with high LDL-C and some of them may have started with a diet able to influence the risk of mortality
No study of unselected people has found an association between TC and degree of atherosclerosis.
in most of the Japanese epidemiological studies, high TC is not a risk factor for stroke, and further, there is an inverse association between TC and all-cause mortality, irrespective of age and sex
have chosen to focus on the association between LDL-C and all-cause and CVD mortality, because mortality has the least risk of bias among all outcome measures.
any beneficial effects of statins on mortality would have been minimal because most statin trials have had little effect on CVD and all-cause mortality, with a maximum reduction of mortality of two percentage points.
ha, thats a academic burn! Side eye on the RR trumpets for small real benefit.
In a recent study, the authors reported that among participants who were older than 65 at baseline, a 30 mg/dL decrease in serum cholesterol was associated with a higher risk of death (HR 1.35, 95% CI 1.18 to 1.54).
So LDL is protective (1.35 HR which is nothing, but the case against LDL is made with LOWER HRs)
this finding suggests that the conventional dietary treatment for high cholesterol with vegetable oil replacing saturated fat may actually increase mortality in those individuals with high LDL-C.
This makes sense, the body makes cholesterol to function, its necessary, a diet that attacks the functioning of cholesterol should have some negative impact on mortality.
Assessments of the association between serum cholesterol and mortality have been studied for decades, and extensive research has shown a weak association between total cholesterol and mortality in the elderly;everal studies have even shown an inverse association.
It is therefore surprising that there is an absence of a review of the literature on mortality and levels of LDL-C, which is routinely referred to as a causal agent in producing CVD 4 and is a target of pharmacological treatment of CVD.
I think this is a direct calling out of pharmacological corruption medicine, but said through a academic lens.
LDL binds to and inactivates a broad range of microorganisms and their toxic products.Diseases caused or aggravated by microorganisms may therefore occur more often in people with low cholesterol, as observed in many studies.
LDL are the firemen in our city, and they go where the fire is, you reduce the firemen your going to have a bad time.
Nine cohort studies including more than 140 000 individuals followed for 10–30 years have found an inverse association between cancer and TC measured at the start of the study, even after excluding deaths that occurred during the first 4 years.
Furthermore, cholesterol lowering experiments on rodents have resulted in cancer
Significantly more patients with cancer have been on cholesterol-lowering treatment.
In agreement with these findings, cancer mortality is significantly lower in individuals with familial hypercholesterolaemia
that LDL-C is lower than normal in patients with acute myocardial infarction
the main goal of prevention of disease is prolongation of life, all-cause mortality is the most important outcome, and is also the most easily defined outcome and least subject to bias.
The shade in this paper!
Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies. Summary:
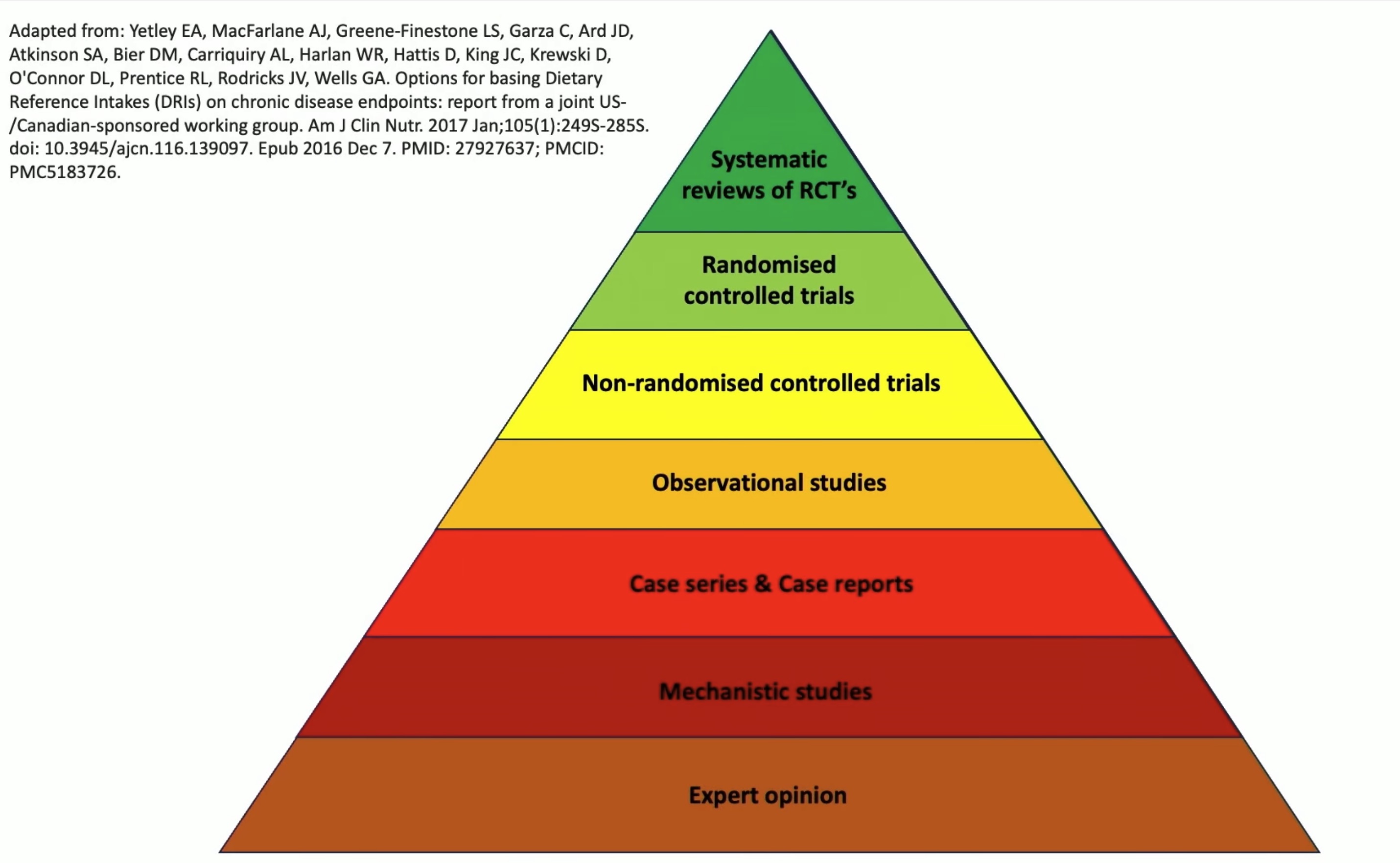
Systematic Review of published cohorts, high value science.
evidence pyramid
.

{kind=link}